


Citation: Narayan A, Salindri AD, Keshavjee S, Muyoyeta M, Velen K, Rueda ZV, et al. (2023) Prioritizing persons deprived of liberty in global guidelines for tuberculosis preventive treatment. PLoS Med 20(10):
e1004288.
https://doi.org/10.1371/journal.pmed.1004288
Published: October 3, 2023
Copyright: © 2023 Narayan et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: The authors received no specific funding for this work.
Competing interests: The spouse of SS was employed by Merck Pharmaceuticals 1997-2007 and retains stock in his retirement account. There is no conflict of interest with the submitted work, but is included in the interest of full disclosure. The other authors have declared that no competing interests exist.
Abbreviations:
HBV,
hepatitis B virus; HCV,
hepatitis C virus; IGRA,
interferon gamma release assay; LMIC,
low- and middle-income country; MDR,
multidrug-resistant; MOUD,
medication for opioid use disorder; PDL,
person deprived of liberty; RR,
rifampicin-resistant; TPT,
tuberculosis preventive treatment; TST,
tuberculin skin test; WHO,
World Health Organization
Summary points
- Persons deprived of liberty (PDLs) are disproportionately impacted by tuberculosis, with high incidence rates and often limited access to diagnostics, treatment, and preventive measures.
- The World Health Organization (WHO) expanded its recommendations for tuberculosis preventive treatment (TPT) to many high-risk populations, but their guidance does not include PDL, and most low- and middle-income countries do not routinely provide TPT in prisons.
- Recent studies demonstrate high acceptability and completion rates of short-course TPT regimens in jails and prisons; costs of these regimens have been markedly reduced through international agreements, making this an opportune for further expanding their use.
- We argue that PDL should be a priority group for TPT in national guidelines and discuss implementation considerations and resource needs for TPT programs in carceral facilities.
- Scaling access to TPT for PDL is important for reducing disease and transmission in this population; it is also critical to advancing an equitable response to tuberculosis.
Tuberculosis continues to be a leading cause of illness and death globally, with greater than 10 million people becoming ill with tuberculosis and 1.6 million deaths estimated to occur each year [1]. The disease disproportionately affects impoverished and socially marginalized populations, with persons deprived of liberty (PDLs) in closed carceral settings having among the highest incidence [2]. Globally, over 10.7 million individuals are held in penal institutions, and several times as many people pass into and out of carceral facilities each year [3]. A recent meta-analysis reported that tuberculosis incidence among PDL was over 10 times higher than that of their surrounding communities [2]. Carceral settings have long been recognized as high-risk settings for tuberculosis disease and transmission. Densely populated by individuals with multiple social and biological risk factors, prison environments are ideal for tuberculosis transmission. Additionally, prisons are severely under resourced, with limited healthcare services, frequently facing shortages of medical staff, and insufficient diagnostic capacity for tuberculosis and related medical comorbidities. Uncontrolled tuberculosis transmission in prisons may amplify epidemics in their surrounding communities, undermining national and regional targets for tuberculosis control [4–6].
In response to the growing evidence reporting the disproportionate burden of tuberculosis faced by PDLs, the World Health Organization (WHO) updated its guidance in 2021 to strongly recommend systematic screening for tuberculosis disease in prisons [7]. Such guidance is critical to ensuring policymakers invest adequately in tuberculosis diagnosis and treatment in carceral facilities [8]. WHO guidelines for tuberculosis preventive treatment (TPT) recently expanded the scope of priority groups for this intervention, however, do not clearly recommend its use in carceral settings [9]. The guidelines only briefly mention prisoners among other risk groups in whom tuberculosis infection testing and treatment “may be considered,” which is a “conditional recommendation” and insufficient to promote policy change. Specific guidance addressing the unique considerations around testing and treatment in carceral settings remain unavailable. Consequently, very few countries with high tuberculosis burden routinely provide tuberculosis infection testing and treatment in prisons. Yet, the case for expanding TPT to PDL has never been stronger. Global estimates for the incidence of tuberculosis in prisons are available for the first time in 2023, documenting a large and growing burden in many regions [10]. Recent studies demonstrate that short-course TPT regimens are associated with high acceptance and completion rates in prisons. A 2022 negotiated agreement markedly reduced the cost of short-course regimens in low- and middle-income countries (LMICs), reducing a key financial barrier [11]. Here, we review and contextualize these developments, discussing their implications along with policy and implementation considerations to inform the design of TPT programs in prisons.
Screening for tuberculosis infection and disease in prisons
Recently published global estimates, leveraging data from more 150 countries, estimated that 125,000 people develop tuberculosis disease in prisons each year, while only 53% are detected and notified [10]. Estimated disease incidence was extremely high in all WHO regions, ranging from 793 cases per 100,000 in the Eastern Mediterranean region to 2,242 cases per 100,000 in the Africa region. In the Americas, the estimated number of tuberculosis cases in prisons has tripled since 2000, amid rising incarceration rates. While fewer data are available concerning the incidence of tuberculosis infections, a recent meta-analysis documented a very high pooled incidence of 15 people acquiring infection per 100 person-years [2]. These high rates of infection point towards an opportunity prevent tuberculosis disease and subsequent transmission using TPT.
A key question for programs providing testing and treatment of tuberculosis infection is the timing of screening. In high tuberculosis–burden communities, and among previously incarcerated individuals, the prevalence of tuberculosis infection is often high, supporting an approach of screening at entry or reentry. By contrast, among individuals incarcerated for the first time in communities with low or moderate tuberculosis incidence, prevalence may be low at entry. For example, a study in Brazil found that <10% of individuals had positive tuberculin skin tests at the time first incarceration but then incurred a>20% annual risk of infection during incarceration [12]. Taken together, these data suggest that screening for tuberculosis infection should be performed at prison entry and periodically to assess for incident infections. In settings with high transmission rates, twice annual screening for incident infections may be needed, with the latter serving to identify recently infected individuals in time to initiate TPT and prevent disease.
Testing for tuberculosis infection may be performed by tuberculin skin tests (TSTs) or interferon gamma release assays (IGRAs); the latter are typically more expensive and require phlebotomy and laboratory equipment. Both approaches, however, confer different advantages with respect to specificity and sensitivity, as well as the need for follow-up. In some high tuberculosis–burden settings, including prisons, programs have elected to forego testing for tuberculosis infection and directly offer preventive treatment to all high-risk individuals [13]. The rationale for this may be multifold: (1) in high transmission settings, the majority of individuals will harbor tuberculosis infection, and the risk of a false negative IGRA/TST is greater, particularly among those with HIV in whom TST has reduced sensitivity; (2) TPT may prevent infections while it is taken, as some clinical trial evidence suggests [14,15]; (3) historical studies in high transmission settings suggested that individuals with negative TSTs were at highest risk of tuberculosis, presumably due to greater susceptibility to initial infection [16]; and (4) the costs of TPT are lower than IGRA testing. Although there have been shortages in tuberculin for TST, new tuberculosis antigen-based skin tests may soon mitigate this problem. The innovation of providing “community-wide” preventive treatment in settings with very high transmission rates is not a new one; some of the earliest isoniazid trials found that community-wide use of preventive treatment was efficacious for individuals with and without infection [17]. Such strategies need to be balanced against risks of adverse events, particularly in populations with medical comorbidities that elevate risk of drug toxicities. Testing for tuberculosis infection must be combined with screening for tuberculosis disease, ideally using both radiography and rapid molecular diagnostics, to identify individuals who require treatment. Many prisons, particularly in LMICs, lack functioning equipment and personnel for performing chest radiography. New, portable chest radiography systems, paired with automated interpretation software, hold promise for making radiography-based screening for disease more accessible in prisons [18,19].
Tuberculosis preventive treatment regimens in carceral settings
With respect to TPT regimens, 6 to 9 months of daily isoniazid (INH) was historically the most commonly used regimen in carceral settings. The effectiveness of this strategy in these settings has been limited, however, due to low treatment acceptance and completion rates. A systematic review of INH-based regimens delivered in carceral settings found a median completion rate of just 44% due to patient and system-level factors [20]. Equally efficacious short-course regimens, including a 3-month (12 weekly dose) regimen of high-dose isoniazid and rifapentine (3HP), have led to markedly improved completion rates in carceral settings compared with 6 or 9 months of isoniazid [21,22]. Two recent studies illustrate successful models for short-course–based TPT in high-burden LMIC prisons. In Malawi and Pakistan, 3HP acceptance in prisons exceeded 95% and completion rates were over 85%, with low rates of adverse events [13,23].
The cost of rifapentine remains one of the major obstacles to adoption and scale-up of short-course TPT regimens in LMICs. UNITAID and its partners brokered a 70% price reduction in 3HP in 2022, with the entire course now available for $14.25 [11]. Such innovations should accelerate 3HP scale-up, yet the manufacturer of this off-patent medication has not made rifapentine routinely available to many countries [24]. Other short-course regimens are also recommended and associated with improved completion rates compared with 6 or 9 months of INH, but, to our knowledge, there are minimal data concerning their use in prisons and jails. These include a 3-month daily regimen of isoniazid and rifampicin and a 4-month daily regimen of rifampicin. Studies are needed to compare adherence, completion, and tolerability, as well as implementation feasibility in prisons, for these daily versus weekly short-course regimens. “Ultra-short-course” regimens, such as the 1-month regimen of daily INH and rifapentine (1HP), appeared noninferior to INH-based regimens among people living with HIV, which has led to a WHO recommendation for their use in this population [25]. Trials assessing 1HP’s effectiveness in individuals without HIV are ongoing. These shorter regimens may increase the likelihood that TPT is completed prior to leaving prisons, which has been a problem with longer regimens.
Challenges and opportunities for tuberculosis preventive treatment in carceral settings
One of the principal challenges to effective delivery of TPT in carceral settings is treatment continuity among individuals leaving the setting, due to interinstitutional transfer or release to the community, which historically resulted in low linkage to care and completion rates [26]. Short-course regimens increase the chance that treatment can be completed before release but have not completely mitigated this problem. Strategies to improve preventive treatment completion have included education, transitional care clinics, and small financial incentives, which have had varying success [27].
In most countries, PDL have higher rates of psychiatric and substance use disorders and related comorbidities, including HIV and chronic hepatitis B virus (HBV) and hepatitis C virus (HCV) infections [28]. These comorbidities are risk factors for adverse events, particularly drug-induced hepatitis from longer regimens, and treatment noncompletion. Testing and treatment for HIV, HBV, and HCV should be integrated with TPT programs, and those with HIV and/or viral hepatitis coinfection may require selection of regimens with lowest risk of liver injury and drug–drug interactions, along with closer monitoring for hepatoxicity. In patients with comorbidities placing them at risk of adverse events from TPT, counseling concerning risks and benefits should be undertaken as part of shared decision-making about whether to initiate treatment. Additionally, substance use and psychiatric disorders should be treated concomitantly; this may include medications for opioid use disorder (MOUDs) for individuals with opioid use disorders. Studies suggest that MOUD substantially improves each step of both the HIV and tuberculosis treatment cascades and have the potential to serve as a bridge to treatment completion after release [29,30]. Because rifampin and rifapentine are potent inducers of cytochrome P450 enzymes and can affect metabolism of opioids and opioid agonists, clinicians should monitor closely during therapy to assess the need for medication adjustments.
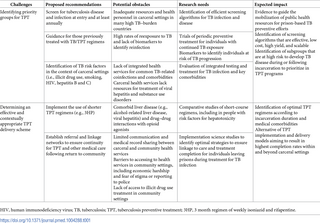
Although treatment of tuberculosis infection has been standard of care in the United States since the early 1960s and the scope of its recommended use was recently broadened by WHO, there continues to be concern about implementing TPT programs among PDL (Table 1). One serious concern is that reinfection following treatment will compromise the effectiveness of the intervention in high-transmission settings, as no tests exist to measure reinfection. Studies among South African gold miners revealed a rapid rebound in tuberculosis incidence within 6 months of completion of TPT [31], and similar patterns could be seen among people who remain incarcerated and exposed to a high force of infection. We note that many individuals in high tuberculosis–burden countries are incarcerated for short sentences, often less than 2 years, such that the exposure to reinfection may be lower. For those who remain incarcerated, prolonged or pulsed preventive treatment may be indicated, though data are mixed. A randomized trial of prolonged (36-month) isoniazid TPT was more effective than 6 months of isoniazid among adults living with HIV in Botswana [15]. Other trials in persons living with HIV found durable effectiveness of 6 months of isoniazid and no superiority of longer durations [32,33]. In a trial conducted in communities in South Africa, Ethiopia, and Mozambique, a repeat round of TPT at 12 months did not confer additional benefits for individuals receiving antiretroviral therapy though the incidence and force of infection in those communities are lower than that of many prisons [34]. Further studies should investigate the potential for continuous or pulsed preventive treatment in high tuberculosis–burden prisons. Finally, TPT programs should be implemented alongside intensive active case finding programs, to reduce transmission and risk of reinfection.
In many settings, the burden of rifampicin-resistant (RR) or multidrug-resistant (MDR) tuberculosis is higher in prisons than in the surrounding communities, with several studies identifying prisons as important drivers of MDR/RR tuberculosis in the broader population [4,35]. While observational studies suggest that fluoroquinolones may be effective as preventive treatment for MDR tuberculosis [36,37], data from randomized trials are still lacking. Randomized trials are currently underway to test the effectiveness of TPT regimens among contacts of people with MDR tuberculosis. While awaiting these data, screening using rapid molecular diagnostics for rifampicin resistance should be performed for contacts of individuals with RR tuberculosis or in prisons with a high prevalence of RR among individuals with newly identified tuberculosis; preventive treatment using fluoroquinolone-based regimens may reduce risk of tuberculosis among these individuals [36].
The path forward: Updating guidelines and national policies for tuberculosis preventive treatment
Preventive treatment remains a crucial but underutilized intervention for reducing the high tuberculosis incidence in carceral settings, particularly in LMICs where the greatest burden occurs. Further, given the dynamic nature of incarceration and high incidence of disease among individuals following release, prevention of tuberculosis in prisons may have outsized benefits for their surrounding communities. Data demonstrating high treatment completion rates for short-course regimens in these settings, together with reductions in the price of rifapentine, make this an opportune moment for expanding access to preventive treatment for PDL. In the absence of international guidance, most countries will not incorporate TPT for PDL into national guidelines and financially prioritize its implementation. Updating and upgrading recommendations for TPT use among PDL, including provision of specific guidance around approaches to testing for infection, screening for disease, and management of medical comorbidities, could provide the foundation for national tuberculosis programs to increase focus on and resources for this population. Given the extraordinarily high incidence of tuberculosis in prisons, such efforts are likely to reduce disparities and advance health equity.
References
- 1.
World Health Organization. Global Tuberculosis Report: 2022. Geneva, Switzerland; 2022. - 2.
Cords O, Martinez L, Warren JL, O’Marr JM, Walter KS, Cohen T, et al. Incidence and prevalence of tuberculosis in incarcerated populations: a systematic review and meta-analysis. Lancet Public Health. 2021;6:e300–e308. pmid:33765455 - 3.
World Prison Brief data | World Prison Brief. [Accessed 2023 Jul 10]. Available from: https://www.prisonstudies.org/world-prison-brief-data - 4.
Warren JL, Grandjean L, Moore DAJ, Lithgow A, Coronel J, Sheen P, et al. Investigating spillover of multidrug-resistant tuberculosis from a prison: a spatial and molecular epidemiological analysis. BMC Med. 2018;16:122. pmid:30071850 - 5.
Walter KS, Martinez L, Arakaki-Sanchez D, Sequera VG, Estigarribia Sanabria G, Cohen T, et al. The escalating tuberculosis crisis in central and South American prisons. Lancet. 2021;397:1591–1596. pmid:33838724 - 6.
Walter KS, dos Santos PCP, Gonçalves TO, da Silva BO, da Silva Santos A, de Cassia Leite A, et al. The role of prisons in disseminating tuberculosis in Brazil: A genomic epidemiology study. Lancet Reg Health Am. 2022;9. pmid:35647574 - 7.
World Health Organization. WHO consolidated guidelines on tuberculosis. Module 2: screening—systematic screening for tuberculosis disease. Geneva: World Health Organization; 2021. - 8.
Charalambous S, Velen K, Rueda Z, Croda J, Herce ME, Shenoi SV, et al. Scaling up evidence-based approaches to tuberculosis screening in prisons. Lancet Public Health. 2023;8:e305–e310. pmid:36780916 - 9.
World Health Organization. WHO consolidated guidelines on tuberculosis. Module 1: prevention–tuberculosis preventive treatment. Geneva, Switzerland; 2020. - 10.
Martinez L, Warren JL, Harries AD, Croda J, Espinal MA, Olarte RAL, et al. Global, regional, and national estimates of tuberculosis incidence and case detection among incarcerated individuals from 2000 to 2019: a systematic analysis. Lancet Public Health. 2023;8:e511–e519. pmid:37393090 - 11.
Partners announce reduced price for patient-friendly tuberculosis preventive treatments. In: Unitaid [Internet]. [Accessed 2023 Jul 10]. Available from: https://unitaid.org/news-blog/tb-preventive-therapy/ - 12.
Carbone A da SS, Paião DSG, Sgarbi RVE, Lemos EF, Cazanti RF, Ota MM, et al. Active and latent tuberculosis in Brazilian correctional facilities: a cross-sectional study. BMC Infect Dis. 2015;15:24. pmid:25608746 - 13.
Jaswal M, Farooq S, Madhani F, Noorani S, Salahuddin N, Amanullah F, et al. Implementing 3HP vs. IPT as TB preventive treatment in Pakistan. Int J Tuberc Lung Dis. 2022;26:741–746. pmid:35898140 - 14.
Rangaka MX, Wilkinson RJ, Boulle A, Glynn JR, Fielding K, van Cutsem G, et al. Isoniazid plus antiretroviral therapy to prevent tuberculosis: a randomised double-blind, placebo-controlled trial. Lancet. 2014;384:682–690. pmid:24835842 - 15.
Samandari T, Agizew TB, Nyirenda S, Tedla Z, Sibanda T, Shang N, et al. 6-month versus 36-month isoniazid preventive treatment for tuberculosis in adults with HIV infection in Botswana: a randomised, double-blind, placebo-controlled trial. Lancet. 2011;377:1588–1598. pmid:21492926 - 16.
Andrews JR, Noubary F, Walensky RP, Cerda R, Losina E, Horsburgh CR. Risk of progression to active tuberculosis following reinfection with Mycobacterium tuberculosis. Clin Infect Dis. 2012;54:784–791. pmid:22267721 - 17.
Comstock GW, Ferebee SH, Hammes LM. A controlled trial of community-wide isoniazid prophylaxis in Alaska. Am Rev Respir Dis. 1967;95:935–943. pmid:6026165 - 18.
Soares TR, Oliveira RD de, Liu YE, Santos A da S, Santos PCPD, Monte , et al. Evaluation of chest X-ray with automated interpretation algorithms for mass tuberculosis screening in prisons: a cross-sectional study. Lancet Reg Health Am. 2023;17:100388. pmid:36776567 - 19.
Velen K, Sathar F, Hoffmann CJ, Hausler H, Fononda A, Govender S, et al. Digital Chest X-ray with Computer-aided Detection for TB Screening within Correctional Facilities. Ann Am Thorac Soc. 2021. pmid:34914539 - 20.
Al-Darraji HAA, Kamarulzaman A, Altice FL. Isoniazid preventive therapy in correctional facilities: a systematic review. Int J Tuberc Lung Dis. 2012;16:871–879. pmid:22410101 - 21.
Juarez-Reyes M, Gallivan M, Chyorny A, O’Keeffe L, Shah NS. Completion Rate and Side-Effect Profile of Three-Month Isoniazid and Rifapentine Treatment for Latent Tuberculosis Infection in an Urban County Jail. Open Forum. Infect Dis Ther. 2016;3:ofv220. pmid:26885547 - 22.
Wheeler C, Mohle-Boetani J. Completion Rates, Adverse Effects, and Costs of a 3-Month and 9-Month Treatment Regimen for Latent Tuberculosis Infection in California Inmates, 2011–2014. Public Health Rep. 2019;134:71S–79S. pmid:31059418 - 23.
Mangochi P, Bossard C, Catacutan C, Van Laeken D, Kwitonda C, Ortuno R, et al. TB screening, prevention and treatment cascade in a Malawi prison. Int J Tuberc Lung Dis 2022;26:956–962. pmid:36163657 - 24.
Guglielmetti L, Günther G, Leu C, Cirillo D, Duarte R, Garcia-Basteiro AL, et al. Rifapentine access in Europe: growing concerns over key tuberculosis treatment component. Eur Respir J 2022;59:2200388. pmid:35589114 - 25.
Swindells S, Ramchandani R, Gupta A, Benson CA, Leon-Cruz J, Mwelase N, et al. One Month of Rifapentine plus Isoniazid to Prevent HIV-Related Tuberculosis. N Engl J Med 2019;380:1001–1011. pmid:30865794 - 26.
Tulsky JP, White MC, Dawson C, Hoynes TM, Goldenson J, Schecter G. Screening for tuberculosis in jail and clinic follow-up after release. Am J Public Health 1998;88:223–226. pmid:9491011 - 27.
White MC, Tulsky JP, Goldenson J, Portillo CJ, Kawamura M, Menendez E. Randomized controlled trial of interventions to improve follow-up for latent tuberculosis infection after release from jail. Arch Intern Med 2002;162:1044–1050. pmid:11996616 - 28.
Dolan K, Wirtz AL, Moazen B, Ndeffo-Mbah M, Galvani A, Kinner SA, et al. Global burden of HIV, viral hepatitis, and tuberculosis in prisoners and detainees. Lancet 2016;388:1089–1102. pmid:27427453 - 29.
Morozova O, Dvoryak S, Altice FL. Methadone treatment improves tuberculosis treatment among hospitalized opioid dependent patients in Ukraine. Int J Drug Policy 2013;24:e91–e98. pmid:24360402 - 30.
Low AJ, Mburu G, Welton NJ, May MT, Davies CF, French C, et al. Impact of Opioid Substitution Therapy on Antiretroviral Therapy Outcomes: A Systematic Review and Meta-Analysis. Clin Infect Dis 2016;63:1094–1104. pmid:27343545 - 31.
Hermans SM, Grant AD, Chihota V, Lewis JJ, Vynnycky E, Churchyard GJ, et al. The timing of tuberculosis after isoniazid preventive therapy among gold miners in South Africa: a prospective cohort study. BMC Med 2016;14:45. pmid:27004413 - 32.
Badje A, Moh R, Gabillard D, Guéhi C, Kabran M, Ntakpé J-B, et al. Effect of isoniazid preventive therapy on risk of death in west African, HIV-infected adults with high CD4 cell counts: long-term follow-up of the Temprano ANRS 12136 trial. Lancet Glob Health 2017;5:e1080–e1089. pmid:29025631 - 33.
Martinson NA, Barnes GL, Moulton LH, Msandiwa R, Hausler H, Ram M, et al. New regimens to prevent tuberculosis in adults with HIV infection. N Engl J Med 2011;365:11–20. pmid:21732833 - 34.
Churchyard G, Cárdenas V, Chihota V, Mngadi K, Sebe M, Brumskine W, et al. Annual Tuberculosis Preventive Therapy for Persons With HIV Infection: A Randomized Trial. Ann Intern Med 2021;174:1367–1376. pmid:34424730 - 35.
Gygli SM, Loiseau C, Jugheli L, Adamia N, Trauner A, Reinhard M, et al. Prisons as ecological drivers of fitness-compensated multidrug-resistant Mycobacterium tuberculosis. Nat Med 2021;27:1171–1177. pmid:34031604 - 36.
Malik AA, Fuad J, Siddiqui S, Amanullah F, Jaswal M, Barry Z, et al. Tuberculosis Preventive Therapy for Individuals Exposed to Drug-resistant Tuberculosis: Feasibility and Safety of a Community-based Delivery of Fluoroquinolone-containing Preventive Regimen. Clin Infect Dis 2020;70:1958–1965. pmid:31190072 - 37.
Bamrah S, Brostrom R, Dorina F, Setik L, Song R, Kawamura LM, et al. Treatment for LTBI in contacts of MDR-TB patients, Federated States of Micronesia, 2009–2012. Int J Tuberc Lung Dis 2014;18:912–918. pmid:25199004
This post was originally published on this site be sure to check out more of their content.



