


Key Points
Question
How does decision-making occur for hospitalized incarcerated persons lacking decisional capacity?
Findings
In this qualitative study of documentation for 43 hospitalized incarcerated persons without decisional capacity, prison employees appeared to have been involved in decisions for half of the admissions, including participating in family meetings and being asked to authorize invasive procedures.
Meaning
In this single-center cohort of hospitalized, incapacitated patients, carceral status appeared to have influenced decision-making practices, representing a threat to autonomy.
Importance
Incarcerated patients admitted to the hospital face threats to their rights to privacy and self-determination in medical decision-making. Little is known about medical decision-making processes for hospitalized incarcerated persons who lack decisional capacity.
Objective
To characterize the prevalence of incapacity among hospitalized incarcerated patients and describe the decision-making processes, including who served as surrogate decision-makers, involvement of prison employees in medical decisions, and ethical concerns emerging from the patients’ care.
Design, Setting, and Participants
Retrospective descriptive and qualitative study of medical records for all patients admitted from prison for at least 24 hours between January 1, 1999, and September 1, 2019, at a large Midwestern academic medical center. Data analysis was performed from March 15, 2021, to December 14, 2022.
Main Outcomes and Measures
Prevalence of prison-to-hospital admissions for patients with a loss of capacity and characteristics of medical decision-making.
Results
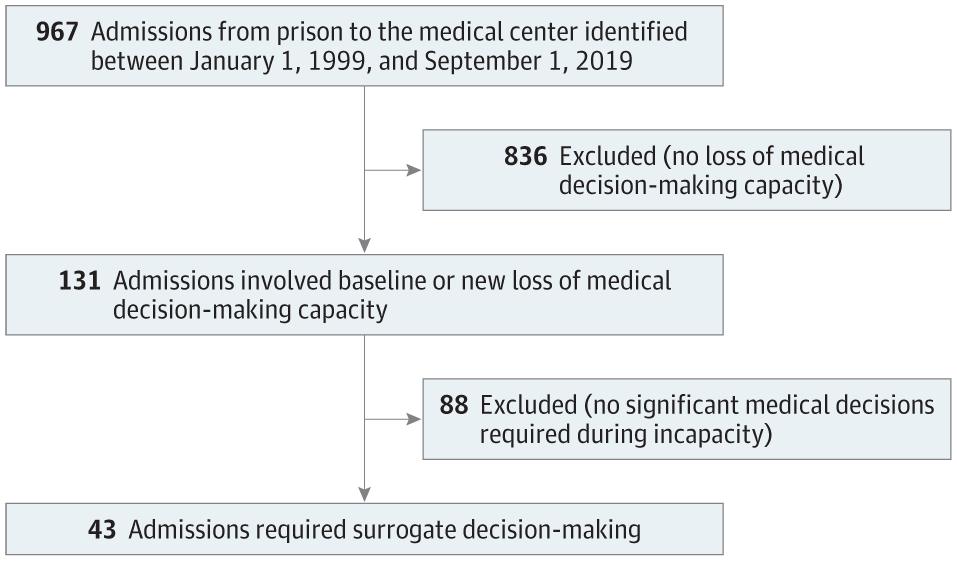
During the 20-year study period, 462 patients from the prison were admitted to the hospital, totaling 967 unique admissions. Of these, 131 admissions (14%) involved patients with a loss of capacity and 43 admissions (4%, representing 34 unique patients) required surrogate decision-making. Ten of these patients had advance directives. Surrogate decision-makers often faced decisions about end-of-life care (n = 17) or procedural consent (n = 23). A family member was identified as surrogate decision-maker in 23 admissions. In 6 cases with a kindred surrogate, additional consent was requested from a prison employee. In total, prison employees were documented as being present during or participating in major medical decisions for half of the admissions. Five themes emerged from thematic analysis: uncertainty and misinformation about patient rights and the role of prison employees in medical decision-making with respect to these two themes, privacy violations, deference to prison officials, and estrangement from family and friends outside of the prison.
Conclusions and Relevance
In this first in-depth description, to date, of decision-making practices for hospitalized incarcerated patients lacking decisional capacity, admissions of these patients generated uncertainty about their rights, sometimes infringing on patients’ privacy and autonomy. Clinicians will encounter incarcerated patients in both hospital and clinic settings and should receive education on how to support ethically and legally sound decision-making practices for this medically vulnerable population.
This post was originally published on this site be sure to check out more of their content.



