



Introduction
Rates of substance use in the United States (US) continue to rise, with the number of individuals endosing past month illicit substance use increasing from approximately 27 million in 2015 to more than 37 million in 2020.1 Nationally representative data indicate that prevalence rates for drug use are generally higher among men than women, although the gender gap in use and SUD in the US has narrowed in recent years.1,2 Among individuals involved in the justice system, the gender gap is reversed with a higher proportion of incarcerated women than men meeting criteria for SUD in both US3 and international samples.4 In the last 40 years, the number of incarcerated women has grown more than six times since 1980,5 an increase of 525%. Driven largely by drug use and drug-related charges, the rate of arrests and incarceration among women has grown two-times that of men, with the rate of drug-related charges increasing more than 200% for women in the past three decades.6 Among US individuals, about half (50.8%) of incarcerated women in prisons are expected to meet SUD criteria for illicit drugs, compared to about a third (38.5%) of men.7 In addition, it estimated that prevalence of SUD among incarcerated women in jail settings is even higher than those in prison.3,8
In recent years, there have been national and international calls for a shift to a public health approach to addressing SUDs rather than a punitive approach.9,10 However, most mind-altering substances remain illegal, which increases the likelihood of significant overlap between substance use and involvement with the criminal justice system. Some criminological theories have attempted to explain the connection between illicit substance use and crime. For example, Canadian and Australian researchers have attempted to understand this relationship using “attributable risk”, which includes asking incarcerated individuals to assess the extent to which their illegal activities were attributed to the need to obtain or maintain their substance use, or if they attribute their commission of illegal activities as being independent of their substance use. This work was expanded to better understand attributable risk by gender among incarcerated individuals. Findings indicated that a higher percentage of women (31%) attributed their illegal activities to substance use compared to men (18%).11 While these studies suggest a strong connection between substance use and crime, gender differences underscore the need for future research on the unique and individualized trajectories of these behaviors which has important implications for SUD treatment in justice system settings.
These trajectories of substance use and crime could also be viewed through the lens of feminist criminology theories including a gendered pathway framework, which indicate that we “must account for the myriad ways that gender matters”.12 This framework suggests that a woman’s criminal behavior (and perhaps criminal career) is often characterized by a history of interconnected experiences with violence and victimization, trauma and mental health issues, problematic and high-risk relationships, and a general lack of social or financial capital.13–15 Because all of these factors are compounded substance use, gendered pathway frameworks also lend themselves to understanding the trajectory of women’s substance use, and the subsequent emerging cycle between substance use and criminal activities.16 Considering the longitudinal nature of these behaviors over time, women’s recovery pathway should also be individualized with the understanding that options for treatment and recovery strategies which “work” for one woman may not be applicable for all women.17
These theoretical perspectives on the intertwined pathways of substance use and criminal activity among women are important in understanding SUD treatment utilization and other services. While research on SUD treatment among justice-involved populations has grown in recent years in the US with rigorously designed, controlled clinical trials on medications to treat opioid use disorder (MOUD),18 and other successful evidence-based practices,19,20 the majority of corrections-based SUD studies have predominantly included incarcerated men or men under community supervision.4,21–23 The purpose of this review is to 1) highlight special considerations for incarcerated women in the US that may serve as facilitating factors or barriers to SUD treatment; 2) describe selected evidence-based practices for women along the cascade of care for SUD including screening and assessment, treatment and intervention strategies, and referral to services during community re-entry; and 3) discuss conclusions and implications.
Special Considerations for Incarcerated Women with SUD
Parenting Status
Incarceration is a stressful and chaotic event for women with children. Parenting responsibilities are often a barrier for women to enter SUD treatment,24 and can be even more of a challenge for incarcerated women. An estimated 57,700 women in US state and federal prisons have minor children.7 The effect of incarceration on both mothers and their children has been documented, and the negative consequences may be even more pronounced for mothers who used substances before incarceration. For example, incarcerated mothers’ separation from their children has been associated with higher rates of depression, anxiety, and tendencies toward self-harm.25,26 Also, when considering the high-risk lifestyles many women may have had before incarceration associated with substance use and criminal behaviors, there may be a considerable amount of shame associated with the stigma of being an incarcerated mother.24,27 In addition, incarceration presents challenges for maintaining a connection with children and attempting to protect them.28,29 Maintaining a connection through regular contact with children is critical and protective for mental health issues among incarcerated women,26 as well as a predictor of successful reunification during community re-entry.30
While studies of pregnant incarcerated women have found similar issues associated with substance use, trauma, and mental health,31 these issues also raise concerns for unborn babies and for treatment opportunities during community transition. For opioid use disorder specifically, Sufrin et al32 found that a majority of US jails and prisons in their sample prescribed MOUD for women who were pregnant, but most prisons and half of the jails only provided continued MOUD community treatment referral rather than the provision of medication. In addition, the majority of prisons (about two-thirds) and jails (about three-fourths) discontinued MOUD following the birth of the baby. While some women may receive better prenatal care in prison than in the community due to poverty, risky lifestyles, and other factors there has been a call in recent years to support standards of care in state and federal correctional facilities for pregnant women with SUD and newborns.31,33,34
There are also a number of negative consequences for children of incarcerated mothers, which may be associated with attachment issues at different developmental stages.35 Incarceration can be traumatic event for children with mothers being removed from the home and children living with a family member or in foster care, including environment stress that may exist before prison due to drug use and other risky lifestyles. While there may be variation in the impact on children and youth associated with maternal incarceration due to many potential factors, substance use in the home and the degree of mother’s problem severity may be critical in the long-term consequences. These findings indicate that SUD treatment for incarcerated women who are pregnant or parenting is critical – not only for them, but also for their children.
Trauma, Victimization, and Co-Occurring Mental Health
A history of trauma is a consistent factor found in the SUD literature among incarcerated women. Among incarcerated women in general, rates of lifetime trauma and victimization among incarcerated women are high,36,37 and rates are even higher among women with a history of substance use.36,38 Research suggests that roughly three-quarters of incarcerated women with SUDs have experienced some form of lifetime traumatic or distressing event.39,40 The rates of victimization and trauma among these women underscores the critical importance of trauma-informed treatments and services incarcerated women with SUDs, which has been consistently reported in the literature.41–43 For example, in one study of perceived treatment needs among incarcerated women, a majority with SUDs reported a need for treatment that included a focus on prior child abuse and domestic violence.39 There is a continued need for efficacious SUD treatment that incorporates the traumatic histories of incarcerated women.
Among justice-involved women with SUD, trauma and violence histories are also often associated with co-occurring mental health issues. For example, one study found that women incarcerated in jail or prison are more likely to report both serious distress and mental health histories compared to men.44 Much like the trajectories associated with substance use and crime, mental health factors are closely associated with substance use for women, potentially increasing their vulnerability for victimization and/or additional distress. Alternatively, some women with trauma histories, experiences of physical pain, or mental health issues may also use illicit substances to cope with stressful situations.
The prevalence of co-occurring mental health issues among incarcerated women was estimated through a meta-analysis at approximately 10.1%.45 Another study of incarcerated women specifically suggested the prevalence rate might be higher at 20%.46 Commonly reported co-occurring disorders (CODs) include anxiety, depression, post-traumatic stress disorder, and bipolar disorder,47,48 although much of the literature has been limited in the number and types of co-occurring mental health disorders assessed.
Despite high prevalence rates, individuals with CODs frequently do not receive treatment in the US,49 and even less for incarcerated women. Nowotny et al46 found that approximately 71% of their sample of incarcerated women with CODs reported receiving no COD treatment in the past year. These low treatment rates for CODs may be due to accessing integrated treatment barriers. Most treatment for incarcerated women with SUDs is primarily aimed at reducing substance use through behavioral interventions like therapeutic communities50 or medications for pregnant women,32 ignoring potential psychiatric problems that may exacerbate substance use and/or contribute to relapse.51 Thus, co-occurring mental health issues, particularly if compounded by trauma and victimization histories, are critical to consider in designing and implementing SUD interventions for incarcerated women.
Health and Transmitted Infections
According to the Centers for Disease Control and Prevention,52 compared to the general population, human immunodeficiency virus (HIV) is three times higher in state and federal prisons. For justice-involved women, the risk for HIV and other blood-borne illnesses is often linked to risky sexual practices before incarceration such as unprotected sex or exchange sex.53,54 For example, one study of incarcerated women in rural Appalachian, more than one-quarter reported having traded sex for drugs, money, or other services in the year before incarceration.55 There is also evidence to support a correlation between arrest and/or incarceration and number of different sexual partners, occurrences of unprotected sex, and concurrent partners.56
Among justice-involved women who use substances, risky sexual practices appear to be even more common.57 For women who have engaged in high-risk drug use (eg, injection and overdose), the risk for blood-borne infections, including both HIV and the hepatitis C virus (HCV) may be further amplified.58 Disease transmission among women who use illicit substances is also intertwined with risky romantic partnerships, with studies pointing to a number of vulnerabilities, such as having a sexual partner who injects drugs or being injected by a partner.59,60
As the rate of women in the justice-system continues to rise,61 incarceration becomes an important opportunity for HIV/HCV prevention efforts, including risk reduction interventions focused on known risk factors.62,63 From community corrections settings to prisons, interventions targeting women most at risk for acquiring HIV/HCV have had positive outcomes.64,65 Furthermore, interventions tailored to focus specifically on the unique needs of women are particularly promising,59,64,66 but research in this area is limited. Thus, SUD treatment interventions for incarcerated women should be designed with an eye toward HIV/HCV and other infectious disease risk reduction.
Race/Ethnicity
Although often unacknowledged in the substance use and crime literature, the potential impact of critical factors such as structural and systemic racism on the financial opportunities, health and health service access, and criminalization of women of color must also be recognized as in understanding criminal activity and justice system involvement.67,68 While there are studies focused on understanding substance use among racial/ethnic minorities, women, and those with criminal justice involvement, there is limited intersectional research investigating substance use among justice-involved women of color.
Bronson et al3 found that, among incarcerated individuals, women and White individuals are more likely to meet criteria for substance use disorders than men and Black or Hispanic individuals. However, other research on justice-involved women specifically found no differences by race among women on lifetime history of substance use disorders.36 Despite these similarities in overall use patterns, the type of SUD which incarcerated women experience may differ by race/ethnicity. The results of one study with incarcerated women suggested that among those who met substance dependence criteria, a higher percentage of Native American women met alcohol and heroin dependence criteria, a higher percentage of Black women met cocaine dependence criteria, and more White women met stimulant dependence criteria.69
Findings related to substance use treatment utilization disparities by race/ethnicity for justice-involved women have shown mixed results. Although some research suggests that White justice-involved individuals are more likely to have been engaged in substance use treatment than people of color in mixed-gender studies,70,71 other studies with justice-involved women did not find race/ethnicity differences in substance use treatment utilization72,73 However, specific treatment needs for justice-involved women of color with SUDs have been documented, such as HIV and sexually transmitted infections (STI) risk74 and race-based stigma surrounding incarceration and substance use.75 These unique patterns of substance use, health risk behaviors, and racial stigma among women of color should be taken into consideration in SUD treatment approaches.
Rural/Urban Populations
Geographic context (living in a rural or urban area) has been shown to be important to understand women’s substance use patterns,76 as well as substance use treatment utilization following release from incarceration.77 Although living in a rural area has traditionally been considered protective for substance use, research has found similar levels of SUD in rural and urban justice-involved women,47 yet rural women access substance use treatment at lower rates than urban women.78 Limited service availability in rural areas is the major reason for this disparity in substance use treatment utilization.79,80 When rural women do access substance use treatment, not all evidenced-based treatment approaches like MOUD are offered.81 In one national study of substance use treatment centers, researchers found that rural treatment centers offered fewer treatment options, had less educated clinical staff, and were less likely to prescribe buprenorphine.82
In addition to the general problem of service availability, rural women face other challenges accessing existing substance use treatment. First, with less comprehensive reentry programs in many rural areas,83 women may be less likely to receive SUD treatment referrals at community reentry. Second, although not a unique barrier to rural women, transportation is more limited and distances to treatment in rural areas are often greater than in urban areas. Public transportation options are fewer, and there is a greater reliance on family and friends for rides, all of which magnify transportation problems for rural women.80,84 Third, other studies have shown that rural women have fewer socioeconomic/employment opportunities80,85 resulting in financial barriers to paying for substance treatment.79
In addition, cultural issues in rural areas may deter women from accessing substance use treatment. Rural communities often promote a culture of self-reliance and distrust of outsiders,86,87 which may make rural women less likely to seek SUD treatment. Rural women tend to have denser social networks, may be more integrated into their communities, and therefore experience less anonymity.88,89 This may make it more difficult to keep their treatment and justice status private, which may subsequently increase the likelihood of experiencing stigma.80,85 Thus, cultural issues in the design and implementation of SUD treatment programs for incarcerated women should include both women of color and women from under-represented geographical areas such as those living in rural communities.
Sexual Orientation and Gender Identity
Sexual orientation and/or gender identity are other considerations among incarcerated women with SUD. This may include women who are of a minority sexual orientation, including lesbian, bisexual, or queer, as well as transgender women. Transgender men and agender and/or non-binary individuals should also be considered, since they may have been assigned female at birth, can share biological features in common with cisgender women, and might at times present as, and/or be perceived as, feminine by others. Within the criminal justice system, housing and classification are most often assigned by biological sex,90 the term “women” is used here to refer to individuals who may identify as women, but also those individuals who may be viewed as women from the perspective of correctional staff.
Within this inclusive definition, the minority stress model91 is a useful theory for understanding SUD treatment considerations for LGBTQ+ women. This theory proposes that sexual minority populations may experience health disparities that are a direct result of persistent individual, interpersonal, and structural stigma which lead to poor health through various psychosocial and physiological mechanisms.92 The framework is supported by research that has consistently documented that LGBTQ+ individuals report higher rates of SUD and related problems when compared to heterosexual and/or cisgender individuals.93–95 Furthermore, although community-based SUD treatment programs which offer tailored services to LGBTQ+ individuals have increased in recent years, treatment options remain limited,96 and even more limited in corrections. Understanding that LGBTQ+ women may also experience additional stress through bias and discrimination in the justice system,97 it is critical that resources are allocated to increasing SUD treatment in carceral settings that are affirming, inclusive, and that offer integrated, trauma-informed care.98
Cascade of Care for Incarcerated Women with SUD
The previous sections have highlighted a number of special considerations for incarcerated women which have been well documented as factors which may facilitate or hinder SUD treatment engagement and retention. The following section is conceptually grounded in the cascade of care framework for SUD treatment. The cascade of care was developed as an organizing framework for the continuum of HIV services from diagnosis, linkage to care, treatment retention, medication receipt, and viral suppression.99 The framework has been applied to SUD treatment by the NIDA-funded Juvenile Justice – Translational Research on Interventions for Adolescents in the Legal System (JJTRIALS) cooperative agreement to assess engagement and retention of juvenile-justice services along the cascade,100,101 as well as to define outcomes for OUD screening/assessment, diagnosis, care linkage, medication initiation, medication retention, and sustained abstinence.102 The cascade of care framework (See Table 1) is used here to overview the literature on SUD screening and assessment, treatment and intervention approaches, and referrals following release of incarcerated women with SUD.
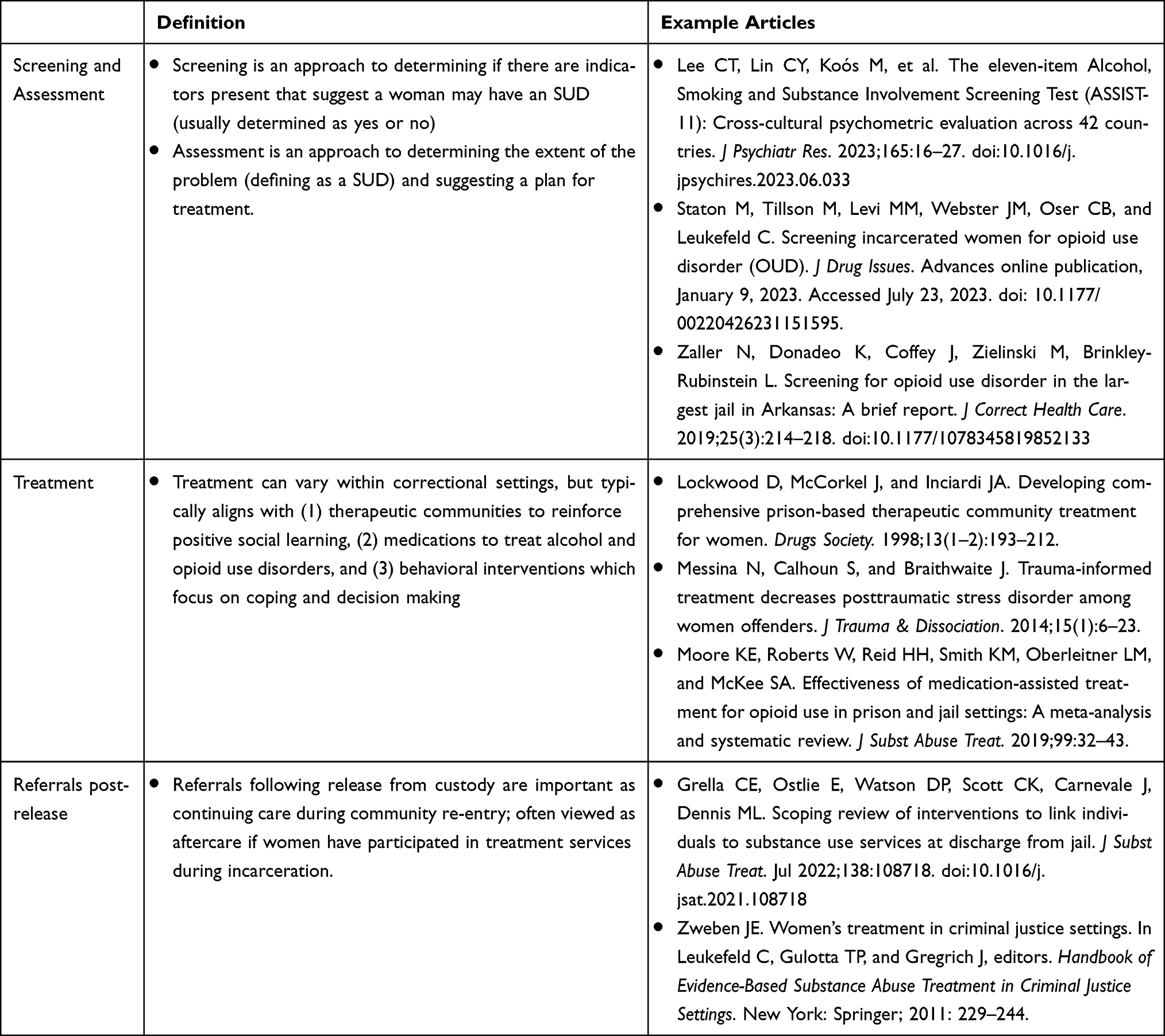 |
Table 1 Overview of the Cascade of Care for SUD Treatment |
SUD Screening and Assessment
One national study showed that more than half prisons surveyed did not include SUD screening and assessment as part of standard intake procedures,103 and these practices were even more limited in county jails.104 Considering the high SUD rates and co-occurring mental health issues among incarcerated women, correctional settings provide important opportunities for SUD screening and assessment and needed linkages to treatment in both carceral settings and during community re-entry. Other settings (eg, health care settings, pharmacies) have adopted evidence-based screening approaches to identify individuals at high risk for SUD, as well as through behavioral trials. World Health Organization (WHO)105 developed and validated the Alcohol Smoking Substance Involvement Screening Test (ASSIST) to identify individuals at risk for substance use disorders in health care settings. The ASSIST was later adapted by the National Institute on Drug Abuse (NIDA) to include separate unique categories of opioid use (prescription opioids vs street opioids), as well as stimulant use (NIDA modified-ASSIST [NM-ASSIST]).106 The NM-ASSIST is quick to administer (5–10 minutes), is easily scored to understand the need for intervention (4+), and has been administered with individuals at high risk for substance use in criminal justice settings.76,107,108 Staton et al107 found that that incarcerated women randomly selected from jails and screened for OUD following a single item to assess past year opioid use reported NM-ASSIST opioid scores that were considerably higher than non-incarcerated samples,109,110 and other samples of incarcerated women.76 The ASSIST has also been validated as a shorter, 11-item scale with individuals across 42 countries and 26 languages.111
The Diagnostic and Statistical Manual (DSM) of Mental Disorders-5 Checklist is another example of an SUD screening tool112 which assesses risk along a list of eleven criteria associated with SUD in the past year with severity ranging from mild to severe,113,114 and a score of two or higher being consistent with a SUD. While widely used as part of a clinical assessment, the DSM SUD Checklist also has utility for SUD screening research. One example is that the DSM SUD Checklist, specifically for opioid use disorder, was used to track symptoms associated with buprenorphine use among patients in primary care.115 Another example is the use of the DSM SUD Checklist to assist with medication tapering among patients in outpatient settings.116 In a recent study with incarcerated women,107 rates of opioid use disorder were high when screened with the DSM-5 OUD Checklist with an average of 10.4 symptoms endorsed before incarceration, with most scoring in the severe range, which was considerably higher than non-incarcerated samples.117 While more commonly used as a clinical component of SUD assessment, the DSM SUD Checklist also has utility for screening among incarcerated women.
SUD Treatment and Interventions
As the population of incarcerated women has grown, so too has a movement for “gender responsive programs”, an umbrella term for services that “understand, recognize, and act upon the unique circumstances that bring many girls and women into the criminal justice system”.12 Gender responsive programs that target the needs of women with SUD remain limited compared to programming for men. The approaches often used are typically “one size fits all” for justice-involved populations and do not embrace women’s relational issues and experiences associated physical and mental health, trauma and victimization, and parenting. In general, evidence-based SUD treatment approaches in the justice system have focused on (1) therapeutic communities to reinforce positive social learning, (2) medications to treat alcohol and opioid use disorders, and (3) behavioral interventions (such as cognitive-behavioral therapies) which focus on coping and decision-making.118 This section will overview selected literature on utilization of each of these approaches with incarcerated women.
A well-established form of SUD treatment for incarcerated individuals is the therapeutic community (TC).119 In general, therapeutic communities are grounded in social learning and modeling which is addressed using confrontational groups, strict enforcement of specific rules, job functions, and other restrictions.120 A specific goal of TC treatment is drugs and/or alcohol abstinence, as well as prosocial behaviors and attitudes, and TC models can be effective with both men and women in correctional settings.50,121 For women in particular, TC programs that incorporate a focus on mental health have also demonstrated significant reductions in substance use, commission of crimes, and improvements in mental health and trauma symptoms following release.122
A more recent shift in corrections-based programming includes the use of medications to treat opioid use disorders (MOUD). While research on MOUD among justice-involved populations has grown in recent years with rigorously designed, controlled clinical trials of buprenorphine, methadone, and extended-release naltrexone, the majority of MOUD studies in corrections include predominantly incarcerated men or men under community supervision, and some do not include women at all.21,22,123 Specifically, Moore et al21 found that in a review on all three forms of FDA-approved OUD medications in jails and prisons found that studies ranged from 60% to 100% male samples, and only one study included only incarcerated women. In addition, most studies examining the effectiveness of MOUD in correctional settings have taken place in prison,123 with the few jail-based studies taking place in large urban areas.124,125 Research is needed on factors associated with MOUD utilization among incarcerated women, both during custody and upon community re-entry.126 In addition, while most research on medications in justice-settings focus on OUD, naltrexone has shown efficacy for alcohol use disorder treatment – yet research with justice involved women is very limited.127 Medications to treat other SUDs are not currently FDA approved. Given the constellation of interrelated issues faced by justice-involved women with SUD, it is also crucial that medications not just be offered in isolation, but in conjunction with other available social/behavioral SUD services, an additional area for future research.
In general, SUD treatment approaches for justice-involved women that integrate trauma-informed interventions have demonstrated positive outcomes.43 One auspicious example of cognitive behavioral therapy for incarcerated women with SUD is Seeking Safety, a co-occurring SUD and post-traumatic stress disorder (PTSD) therapy which utilizes psychoeducation and coping skills.128,129 Seeking Safety has been used as an enhancement to prison-based SUD treatment and shown to reduce symptoms of PTSD and other mental health issues among women with SUD over time.43,128,130–134 While outcomes of studies implementing Seeking Safety have been promising, additional research is needed specifically in conjunction with SUD treatment for women to further verify effectiveness. Other examples of interventions using cognitive behavioral approaches in the co-treatment of SUD and violence include Helping Women Recover135 and Beyond Trauma.136 These findings suggest that the co-treatment of trauma and SUD is critical for incarcerated women.
A more recently developing body of cognitive interventions for women include mindfulness, an approach focused on skill building to be more aware of one’s experiences to create an open, accepting, and non-reactive awareness.19 Mindfulness-based interventions have shown promise in the reduction of mental health symptoms among incarcerated women137 and women in residential SUD treatment programs.20
Regardless of the specific treatment approach, carceral settings provide a critical timepoint to offer programs that address women’s interrelated needs of substance use and criminal activity. Gender-responsive programs, in principle, should address women’s specific needs, including substance use, mental health, trauma, significant relationships, as well as self-sufficiency. However, these treatment opportunities may be limited in corrections since they can be costly and burdensome to implement, requiring more time and energy from staff, both in training and service delivery.138,139 Thus, despite SUD and co-occurring issues among incarcerated women, treatment opportunities, particularly with a gender-responsive framework, are too often limited.
Referrals and Linkages to Community Care for Women After Release
Due to the limited corrections-based SUD treatment availability for women, referrals are often made to community “aftercare” programs following release from custody.140 Community treatment programs should employ “wraparound services” or a “continuum of care” from the correctional setting to the community to ensure that women’s often-interrelated issues are “simultaneously and successively” addressed,139 to promote a sense of safety, connection, and empowerment.141 A specific goal is to provide linkages to community resources to maintain long term therapeutic relationships to support SUD recovery. The chronic nature of substance use underscores the on-going need for continuity of care for individuals reentering the community following incarceration. While substance use problem severity is broadly linked to recidivism,142,143 relapse to substance use during community reentry is highly related to an increased likelihood of overdose.144 Women re-entering the community following jail or prison release are more vulnerable to overdose during the reentry period than men145 or women in the general population.144 Risk of relapse during the reentry period and the associated overdose risk may be further complicated by the vulnerabilities experienced by women both before, and following incarceration (eg, mental health problems, parenting-related stress, and history of victimization).44,146,147 These vulnerabilities are an important consideration when connecting women to community care, and interventions that address these needs holistically are critical in ensuring positive reentry outcomes for women, including risk reduction of relapse and/or overdose.
To more fully address the needs of women with SUD, studies have pointed to the role of community recovery support services during re-entry in achieving positive behavior change, as these services can improve access to needed social and environmental supports.148 For those reentering the community following incarceration, peer support specialists appear to be especially beneficial because of their lived experiences with navigating the challenges of reintegrating into society following incarceration, including understanding the demands for those with community correction requirements.149,150 Furthermore, peer support specialists serve as a source of accountability during reentry151 while also providing clients support in addressing basic needs such as employment, transportation, and housing.149 Heidemann et al152 examined support sources for formerly incarcerated women and reported that support from “others” (peers, agency staff, other professionals) significantly predicted women’s life satisfaction, as opposed to friends/family. These findings have been echoed elsewhere, with peer support specialists recognizing their role in linkages to care for women at community re-entry.153
Peers may be one component of an integral stable social support network for women during community reentry. Strengthening women’s positive support networks (family, partners) has increasingly become a focus of many reentry programs.154 For women who use drugs, establishing new, non-drug using social network may aid in sustaining recovery,155 and thus, improve the likelihood of positive reentry outcomes. Parole officers can also play an important supportive role to women at reentry,156,157 as can other strategies such as case management, medical management, motivation-based interventions, peer navigation or some combination thereof.140 Much like the broader treatment literature, few re-entry programs have been designed for women, including those focusing on SUD.158 In a scoping review of substance use service linkage interventions for individuals reentering the community from jail, Grella et al140 found that only 2 of the 14 included women-specific components, which is clearly a critical area of needed future research.
Conclusions and Implications
In conclusion, this review indicates that there is a disproportionate representation of women with SUD in the criminal justice system in the US, and they have a number of unique issues related to SUD treatment engagement and retention. As the numbers of incarcerated women have continued to rise in recent years, SUD screening and treatment opportunities need to be standardized and expanded in both carceral settings and during community re-entry. In the absence of consistent and standardized evidence-based SUD screening and assessment tools, women who may benefit from services may pass through the justice system unrecognized, missing a critical opportunity for intervention. If implemented on a broad scale, screening tools may be effective in identifying more women with service needs during incarceration.
Also, gender-responsive treatment approaches are often limited in corrections, oftentimes because the number of women is smaller. Increasing opportunities for treatment for justice-involved women is important, but must be done with an eye to meeting specific needs which may vary by demographics (race/ethnicity, living environment, sexual orientation/gender identity), and mental and physical health issues including anxiety, depression, and PTSD related to violence and victimization histories. It is also noteworthy that most incarcerated women have children, and SUD treatment must incorporate a focus on issues associated with reunification with their children, efforts to increase parenting skills, and providing support for children. Women’s success in SUD treatment depends on addressing these needs to support treatment success.
Incarceration and community re-entry are stressful, and being attentive to women’s needs associated with their families, relationships, and social networks is critical to success. Given that women’s patterns of substance use, periods of abstinence, and occurrences of relapse are closely tied to their intimate partner relationships, it is also important that corrections-based treatment provides an emphasis on social relationships and connectedness following release.59 In addition to programs during custody, there is a need for community re-entry planning and “warm-handoff” to community-based services for all women following release, but particularly important for women returning to rural communities with limited service availability.
We recognize that this review is limited to US studies with justice-involved women, which may limit generalizability of findings to women with SUD incarcerated in other countries. While beyond the scope of work for this review, attention to variations in criminal justice systems and the nature of SUD programming in other countries should be considered in future research. This review has important implications for US correctional policies to continue to support and expand evidence-based practices along the cascade of care continuum. Attrition can occur during each phase from engagement to retention, and it is vital that correctional contexts support successful progression through each phase to support positive recovery outcomes. With an increase in treatment availability and access, there should also be a focus among correctional and community treatment leadership on stigma reduction when women re-enter the community including education, referrals to an array of service providers, and family-supportive services and resources.
There are also implications for expanding corrections-based MOUD treatment for women. Studies have shown benefits of MOUD initiation during custody including significant (85%) reductions in drug-related overdose in the month after prison release159 and reductions in recidivism.160 However, MOUD remains widely underutilized in correction settings, particularly for women.21,22,123 Implications for research include increasing our understanding of MOUD use among women, advancing research on medications to treat other SUDs, short and long-term MOUD outcomes in custody and during community transition, and necessary wraparound services to increase the likelihood of MOUD retention.
Other implications of this review include the need for expanded access to supportive recovery resources during community re-entry to prevent relapse and overdose. Relapse after incarceration-induced abstinence is associated with an exponential increase in overdose fatality.161–163 Because women with SUD experience unique structural and social vulnerabilities that impact both relapse and overdose risk (eg, drug-involved romantic relationships, interpersonal violence, lifetime adverse experiences, poor mental health, parenting-related stress, and unequal gendered power dynamics)146,147,164,165 interventions that address these types of underlying factors are critical in having a long-term, sustainable impact on successful recovery among women.
Funding
This research was supported by Justice Community Opioid Innovation Network (JCOIN) grant to the University of Kentucky (UG1DA050069), which is funded by the National Institute on Drug Abuse as part of the NIH HEAL Initiative. The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official views of the NIH, the NIH HEAL Initiative, or the participating JCOIN sites.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Center for Behavioral Health Statistics and Quality (CBHSQ). Results from the 2020 National Survey on Drug Use and Health: detailed tables. U.S. Department of Health & Human Services, Substance Abuse and Mental Health Services Administration; 2021. Available from: https://www.samhsa.gov/data/report/2020-nsduh-detailed-tables.
2. Pitel L, Geckova AM, van Dijk JP, Reijneveld SA. Gender differences in adolescent health-related behaviour diminished between 1998 and 2006. Public Health. 2010;124(9):512–518. doi:10.1016/j.puhe.2010.05.005
3. Bronson J, Stroop J, Zimmer S, Berzofsky M. Drug use, dependence, and abuse among state prisoners and jail inmates, 2007–2009. U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics; 2017. Available from: https://bjs.ojp.gov/content/pub/pdf/dudaspji0709.pdf.
4. Fazel S, Yoon IA, Hayes AJ. Substance use disorders in prisoners: an updated systematic review and meta-regression analysis in recently incarcerated men and women. Addict. 2017;112(10):1725–1739. doi:10.1111/add.13877
5. Monazzam N, Budd KM. Incarcerated women and girls. The Sentencing Project; April 3, 2023. Available from: https://www.sentencingproject.org/fact-sheet/incarcerated-women-and-girls/.
6. Herring T. Since you asked: what role does drug enforcement play in the rising incarceration of women; November 10, 2020. Available from: https://www.prisonpolicy.org/blog/2020/11/10/women-drug-enforcement/.
7. Maruschak LM, Bronson J, Alper M. Alcohol and drug use and treatment reported by prisoners. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics; 2021. Available from: https://www.ojp.gov/library/publications/alcohol-and-drug-use-and-treatment-reported-prisoners-survey-prison-inmates.
8. Swavola E, Riley K, Subramanian R. Overlooked: women and jails in an era of reform. Vera Institute of Justice; August, 2016. Available from: https://www.vera.org/publications/overlooked-women-and-jails-report.
9. Volkow ND, Poznyak V, Saxena S, Gerra G. for UNODC-WHO Informal International Scientific Network. Drug use disorders: impact of a public health rather than a criminal justice approach. World Psychiatry. 2017;16(2):213–214. doi:10.1002/wps.20428
10. Volkow ND. Addiction should be treated, not penalized. Neuropsychopharmacology. 2021;46(12):2048–2050. doi:10.1038/s41386-021-01087-2
11. Johnson H. Drugs and crime: a study of incarcerated female offenders. Australian Research Institute, Research and Public Policy. Series No. 63; 2004. Available from: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.498.8926&rep=rep1&type=pdf.
12. Chesney-Lind M, Pasko L, editors. The Female Offender: Girls, Women, and Crime.
13. Leverentz AM. The Ex-Prisoner’s Dilemma: How Women Negotiate Competing Narratives of Reentry and Desistance. New Brunswick, NJ: Rutgers University Press; 2014.
14. Visher CA, Travis J. Transitions from prison to community: understanding individual pathways. Annu Rev Sociol. 2003;29(1):89–113. doi:10.1146/annurev.soc.29.010202.095931
15. Wesely J, Dewey S. Confronting gendered pathways to incarceration: considerations for reentry programming. Soc Justice. 2018;45(1):57–82.
16. Salisbury EJ, Van Voorhis P. Gendered pathways: a quantitative investigation of women probationers’ paths to incarceration. Crim Justice Behav. 2009;36(6):541–566. doi:10.1177/0093854809334076
17. White W, Kurtz E. The varieties of recovery experience. Int J Self Help Self Care. 2006;3(1–2):21–61. doi:10.2190/911R-MTQ5-VJ1H-75CU
18. Lim S, Cherian T, Katyal M, et al. Association between jail‐based methadone or buprenorphine treatment for opioid use disorder and overdose mortality after release from New York City jails 2011–17. Addict. 2023;118(3):459–467. doi:10.1111/add.16071
19. Amaro H, Black DS. Mindfulness-based intervention effects on substance use and relapse among women in residential treatment: a randomized controlled trial with 8.5-month follow-up period from the moment-by-moment in women’s recovery project. Psychosom Med. 2021;83(6):528. doi:10.1097/PSY.0000000000000907
20. Black DS, Amaro H. Moment-by-Moment in Women’s Recovery (MMWR): mindfulness-based intervention effects on residential substance use disorder treatment retention in a randomized controlled trial. Behav Res Ther. 2019;120:103437. doi:10.1016/j.brat.2019.103437
21. Moore KE, Roberts W, Reid HH, Smith KM, Oberleitner LM, McKee SA. Effectiveness of medication assisted treatment for opioid use in prison and jail settings: a meta-analysis and systematic review. J Subst Abuse Treat. 2019;99:32–43. doi:10.1016/j.jsat.2018.12.003
22. Sharma A, O’Grady KE, Kelly SM, et al. Pharmacotherapy for opioid dependence in jails and prisons: research review update and future directions. Subst Abuse Rehabil. 2016;7(1):27–40. doi:10.2147/SAR.S81602
23. Newbury-Birch D, Ferguson J, Landale S, et al. A systematic review of the efficacy of alcohol interventions for incarcerated people. Alcohol Alcohol. 2018;53(4):412–425. doi:10.1093/alcalc/agy032
24. Choi S, Rosenbloom D, Stein M, Raifman J, Clark J. Differential gateways, facilitators, and barriers to substance use disorder treatment for pregnant women and mothers: a scoping systematic review. J Addict Med. 2022;16(3):e185–e196. doi:10.1097/ADM.0000000000000909
25. Milavetz Z, Pritzl K, Muentner L, Poehlmann‐Tynan J. Unmet mental health needs of jailed parents with young children. Fam Relat. 2021;70(1):130–145. doi:10.1111/fare.12525
26. Stanton AE, Rose SJ. The mental health of mothers currently and formerly incarcerated in jails and prisons: an integrative review on mental health, mental health treatment, and traumatic experiences. J Forensic Nurs. 2020;16(4):224–231. doi:10.1097/JFN.0000000000000302
27. Murray J, Murray L. Parental incarceration, attachment and child psychopathology. Attach Hum Dev. 2010;12(4):289–309. doi:10.1080/14751790903416889
28. Fowler C, Rossiter C, Power T, Dawson A, Jackson D, Roche MA. Maternal incarceration: impact on parent–child relationships. J Child Health Care. 2022;26(1):82–95. doi:10.1177/13674935211000882
29. Sapkota D, Dennison S, Allen J, et al. Navigating pregnancy and early motherhood in prison: a thematic analysis of mothers’ experiences. Health Justice. 2022;10(1):32. doi:10.1186/s40352-022-00196-4
30. Tuerk EH, Loper AB. Contact between incarcerated mothers and their children: assessing parenting stress. J Offender Rehabil. 2006;43(1):23–43. doi:10.1300/J076v43n01_02
31. Nair S, McGreevy JE, Hutchinson-Colas J, Turock H, Chervenak F, Bachmann G. Pregnancy in incarcerated women: need for national legislation to standardize care. J Perinat Med. 2021;49(7):830–836. doi:10.1515/jpm-2021-0145
32. Sufrin C, Sutherland L, Beal L, Terplan M, Latkin C, Clarke JG. Opioid use disorder incidence and treatment among incarcerated pregnant women in the United States: results from a national surveillance study. Addict. 2020;115(11):2057–2065. doi:10.1111/add.15030
33. Kelsey CM, Medel N, Mullins C, Dallaire D, Forestell C. An examination of care practices of pregnant women incarcerated in jail facilities in the United States. Matern Child Health J. 2017;21:1260–1266. doi:10.1007/s10995-016-2224-5
34. Kramer C, Thomas K, Patil A, Hayes CM, Sufrin CB. Shackling and pregnancy care policies in US prisons and jails. Matern Child Health J. 2023;27(1):186–196. doi:10.1007/s10995-022-03526-y
35. Herreros-Fraile A, Carcedo RJ, Viedma A, et al. Parental incarceration, development, and well-being: a developmental systematic review. Int J Environ Res Public Health. 2023;20(4):3143. doi:10.3390/ijerph20043143
36. Green BL, Dass-Brailsford P, Hurtado de Mendoza A, et al. Trauma experiences and mental health among incarcerated women. Psychol Trauma. 2016;8(4):455–463. doi:10.1037/tra0000113
37. Karlsson ME, Zielinski MJ. Sexual victimization and mental illness prevalence rates among incarcerated women: a literature review. Trauma Violence Abuse. 2020;21(2):326–349. doi:10.1177/1524838018767933
38. Gil-Rivas V, Prause J, Grella CE. Substance use after residential treatment among individuals with co-occurring disorders: the role of anxiety/depressive symptoms and trauma exposure. Psychol Addict Behav. 2009;23(2):303–314. doi:10.1037/a0015355
39. Lynch SM, Fritch A, Heath NM. Looking beneath the surface: the nature of incarcerated women’s experiences of interpersonal violence, treatment needs, and mental health. Fem Criminol. 2012;7(4):381–400. doi:10.1177/1557085112439224
40. Scott CK, Dennis ML, Lurigio AJ. Comorbidity among female detainees in drug treatment: an exploration of internalizing and externalizing disorders. Psychiatr Rehabil J. 2015;38(1):35–44. doi:10.1037/prj0000134
41. Fuentes CM. Nobody’s child: the role of trauma and interpersonal violence in women’s pathways to incarceration and resultant service needs. Med Anthropol Q. 2014;28(1):85–104. doi:10.1111/maq.12058
42. Kubiak S, Covington S, Hillier C. Trauma-informed corrections. In: Springer D, Roberts A, editors. Social Work in Juvenile and Criminal Justice System.
43. King EA. Outcomes of trauma-informed interventions for incarcerated women: a review. Int J Offender Ther Comp Criminol. 2017;61(6):667–688. doi:10.1177/0306624X15603082
44. Bronson J, Berzofsky M. Indicators of mental health problems reported by prisoners and jail inmates, 2011–2012. U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics; 2017. Available from: https://www.bjs.gov/content/pub/pdf/imhprpji1112.pdf.
45. Baranyi G, Fazel S, Langerfeldt SD, Mundt AP. The prevalence of comorbid serious mental illnesses and substance use disorders in prison populations: a systematic review and meta-analysis. Lancet Public Health. 2022;7(6):e557–e568. doi:10.1016/S2468-2667(22)00093-7
46. Nowotny KM, Belknap J, Lynch S, DeHart D. Risk profile and treatment needs of women in jail with co-occurring serious mental illness and substance use disorders. Women Health. 2014;54(8):781–795. doi:10.1080/03630242.2014.932892
47. Lynch SM, Dehart DD, Belknap JE, et al. A multisite study of the prevalence of serious mental illness, PTSD, and substance use disorders of women in jail. Psychiatr Serv. 2014;65(5):670–674. doi:10.1176/appi.ps.201300172
48. Zlotnick C, Clarke JG, Friedmann PD, Roberts MB, Sacks S, Melnick G. Gender differences in comorbid disorders among offenders in prison substance abuse treatment programs. Behav Sci Law. 2008;26(4):403–412. doi:10.1002/bsl.831
49. Bose J, Hedden SL, Lipari RN, Park-Lee E, Porter JD, Pemberton MR. Key substance abuse indicators in the United States: results from the 2015 National Survey on Drug Use and Health. Substance Abuse and Mental Health Services Administration; 2016. Available from: https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2015/NSDUH-FFR1-2015/NSDUH-FFR1-2015.htm.
50. Hall EA, Prendergast ML, Wellisch J, Patten M, Cao Y. Treating drug-abusing women prisoners: an outcomes evaluation of the Forever Free program. Prison J. 2004;84(1):81–105. doi:10.1177/0032885503262456
51. Johnson JE, Schonbrun YC, Peabody ME, et al. Provider experiences with prison care and aftercare for women with co-occurring mental health and substance use disorders: treatment, resource, and systems integration challenges. J Behav Health Serv Res. 2015;42(4):417–436. doi:10.1007/s11414-014-9397-8
52. Centers for Disease Control and Prevention. Data and Statistics. Correctional Health; April 24, 2023. Available from: https://www.cdc.gov/correctionalhealth/health-data.html#:~:text=the%20general%20population.-,HIV,in%20the%20general%20U.S.%20population.
53. Loeliger KB, Biggs ML, Young R, et al. Gender differences in HIV risk behaviors among persons involved in the U.S. criminal justice system and living with HIV or at risk for HIV: a “seek, test, treat, and retain” harmonization consortium. AIDS Behav. 2017;21(10):2945–2957. doi:10.1007/s10461-017-1722-9
54. Tillson M, Strickland JC, Staton M. Age of first arrest, sex, and drug use as correlates of adult risk behaviors among rural women in jails. Women Crim Justice. 2017;27(5):287–301. doi:10.1080/08974454.2017.1291392
55. Dickson MF, Tillson M, Calvert JM, Staton M. Transactional sex among rural, justice-involved Appalachian women who use drugs. J Rural Health. 2023;39(4):789–794. doi:10.1111/jrh.12741
56. Knittel AK, Lambdin BH, Comfort ML, Kral AH, Lorvick J. Sexual risk and criminal justice involvement among women who use drugs. AIDS Behav. 2019;23(12):3366–3374. doi:10.1007/s10461-019-02447-2
57. Slavin MN, Hochstatter K, Kraus SW, Earleywine M, El-Bassel N. Associations between cannabis use and sexual risk behavior among women under community supervision: a brief report. Int J Sex Health. 2021;33(2):123–130. doi:10.1080/19317611.2020.1864558
58. Lorvick J, Comfort M, Kral AH, Lambdin BH. Exploring lifetime accumulation of criminal justice involvement and associated health and social outcomes in a community-based sample of women who use drugs. J Urban Health. 2018;95(4):584–593. doi:10.1007/s11524-017-0204-8
59. Staton M, Strickland JC, Webster JM, Leukefeld C, Oser C, Pike E. HIV prevention in rural Appalachian jails: implications for re-entry risk reduction among women who use drugs. AIDS Behav. 2018;22(12):4009–4018. doi:10.1007/s10461-018-2209-z
60. Young AM, Larian N, Havens JR. Gender differences in circumstances surrounding first injection experience of rural injection drug users in the United States. Drug Alcohol Depend. 2014;134:401–405. doi:10.1016/j.drugalcdep.2013.10.013
61. Sawyer W. The gender divide: tracking women’s state prison growth. Prison Policy Initiative; January 9, 2018. Available from: https://www.prisonpolicy.org/reports/women_overtime.html.
62. El-Bassel N, Marotta PL, Shaw SA, et al. Women in community corrections in New York City: HIV infection and risks. Int J STD AIDS. 2017;28(2):160–169. doi:10.1177/0956462416633624
63. Strickland JC, Staton M, Leukefeld CG, Oser CB, Webster JM. Hepatitis C antibody reactivity among high-risk rural women: opportunities for services and treatment in the criminal justice system. Int J Prison Health. 2018;14(2):89–100. doi:10.1108/IJPH-03-2017-0012
64. Fogel CI, Crandell JL, Neevel AM, et al. Efficacy of an adapted HIV and sexually transmitted infection prevention intervention for incarcerated women: a randomized controlled trial. Am J Public Health. 2015;105(4):802–809. doi:10.2105/AJPH.2014.302105
65. Gilbert L, Goddard-Eckrich D, Hunt T, et al. Efficacy of a computerized intervention on HIV and intimate partner violence among substance-using women in community corrections: a randomized controlled trial. Am J Public Health. 2016;106(7):1278–1286. doi:10.2105/AJPH.2016.303119
66. Knudsen HK, Staton-Tindall M, Oser CB, Havens JR, Leukefeld CG. Reducing risky relationships: a multisite randomized trial of a prison-based intervention for reducing HIV sexual risk behaviors among women with a history of drug use. AIDS Care. 2014;26(9):1071–1079. doi:10.1080/09540121.2013.878779
67. Bailey ZD, Feldman JM, Bassett MT. How structural racism works: racist policies as a root Cause of U.S. racial health inequities. N Engl J Med. 2021;384(8):768–773. doi:10.1056/NEJMms2025396
68. Powell AJ, Phelps MS. Gendered racial vulnerability: how women confront crime and criminalization. Law Soc Rev. 2021;55(3):429–451. doi:10.1111/lasr.12561
69. Proctor SL. Substance use disorder prevalence among female state prison inmates. Am J Drug Alcohol Abuse. 2012;38(4):278–285. doi:10.3109/00952990.2012.668596
70. Hedden BJ, Comartin E, Hambrick N, Kubiak S. Racial disparities in access to and utilization of jail- and community-based mental health treatment in 8 US midwestern jails in 2017. Am J Public Health. 2021;111(2):277–285. doi:10.2105/AJPH.2020.305992
71. Nowotny KM. Race/ethnic disparities in the utilization of treatment for drug dependent inmates in U.S. state correctional facilities. Addict Behav. 2015;40:148–153. doi:10.1016/j.addbeh.2014.09.005
72. Jordan BK, Federman EB, Burns BJ, Schlenger WE, Fairbank JA, Caddell JM. Lifetime use of mental health and substance abuse treatment services by incarcerated women felons. Psychiatr Serv. 2002;53(3):317–325. doi:10.1176/appi.ps.53.3.317
73. Timko C, Johnson JE, Kurth M, Schonbrun YC, Anderson BJ, Stein MD. Health services use among jailed women with alcohol use disorders. J Behav Health Serv Res. 2019;46(1):116–128. doi:10.1007/s11414-018-9634-7
74. Mahaffey C, Stevens-Watkins D, Knighton JS. Psychosocial determinants of health among incarcerated Black women: a systematic literature review. J Health Care Poor Underserved. 2016;27(2A):45–70. doi:10.1353/hpu.2016.0059
75. Gunn AJ, Sacks TK, Jemal A. ”That’s not me anymore”: resistance strategies for managing intersectional stigmas for women with substance use and incarceration histories. Qual Soc Work. 2018;17(4):490–508. doi:10.1177/1473325016680282
76. Staton M, Ciciurkaite G, Oser C, et al. Drug use and incarceration among rural Appalachian women: findings from a jail sample. Subst Use Misuse. 2018;53(6):931–941. doi:10.1080/10826084.2017.1385631
77. Willging CE, Nicdao EG, Trott EM, Kellett NC. Structural inequality and social support for women prisoners released to rural communities. Women Crim Justice. 2016;26(2):145–164. doi:10.1080/08974454.2015.1067174
78. Staton-Tindall M, McNees E, Leukefeld C, et al. Treatment utilization among metropolitan and nonmetropolitan participants of corrections-based substance abuse programs reentering the community. J Soc Serv Res. 2011;37(4):379–389. doi:10.1080/01488376.2011.582019
79. Browne T, Priester MA, Clone S, Iachini A, DeHart D, Hock R. Barriers and facilitators to substance use treatment in the rural south: a qualitative study. J Rural Health. 2016;32(1):92–101. doi:10.1111/jrh.12129
80. Zajac G, Hutchison R, Meyer CA. An examination of rural prisoner reentry challenges. Harrisburg, PA: Center for Rural Pennsylvania; 2014. Available from: https://cjrc.la.psu.edu/wp-content/uploads/sites/21/2020/10/CRPA-Rural-Reentry-Report-Final-Justice-Center-version.pdf.
81. Lister JJ, Weaver A, Ellis JD, Himle JA, Ledgerwood DM. A systematic review of rural-specific barriers to medication treatment for opioid use disorder in the United States. Am J Drug Alcohol Abuse. 2020;46(3):273–288. doi:10.1080/00952990.2019.1694536
82. Edmond MB, Aletraris L, Roman PM. Rural substance use treatment centers in the United States: an assessment of treatment quality by location. Am J Drug Alcohol Abuse. 2015;41(5):449–457. doi:10.3109/00952990.2015.1059842
83. Scroggins JR, Malley S. Reentry and the (unmet) needs of women. J Offender Rehabil. 2010;49(2):146–163. doi:10.1080/10509670903546864
84. Staton M, Pike E, Tillson M, Lofwall MR. Facilitating factors and barriers for use of medications to treat opioid use disorder (MOUD) among justice‐involved individuals in rural Appalachia. J Community Psychol. 2023. doi:10.1002/jcop.23029
85. Beichner D, Rabe-Hemp C. “I don’t want to go back to that town:” Incarcerated mothers and their return home to rural communities. Crit Criminol. 2014;22:527–543. doi:10.1007/s10612-014-9253-4
86. Lichter DT, Ziliak JP. The rural-urban interface: new patterns of spatial interdependence and inequality in America. Ann Am Acad Political Soc Sci. 2017;672(1):6–25. doi:10.1177/0002716217714180
87. Moody LN, Satterwhite E, Bickel WK. Substance use in rural Central Appalachia: current status and treatment considerations. J Rural Ment Health. 2017;41(2):123–135. doi:10.1037/rmh0000064
88. Keyes KM, Cerda M, Brady JE, Havens JR, Galea S. Understanding the rural-urban differences in nonmedical prescription opioid use and abuse in the United States. Am J Public Health. 2014;104(2):e52–9. doi:10.2105/AJPH.2013.301709
89. Tillson M, Dickson MF, Webster JM, Staton M. Community relationship quality and reincarceration following rural drug-using women’s reentry from jail. Crim Just Behav. 2022;49(6):853–871. doi:10.1177/00938548211073603
90. Ledesma E, Ford CL. Health Implications of housing assignments for incarcerated transgender women. Am J Public Health. 2020;110(5):650–654. doi:10.2105/AJPH.2020.305565
91. Meyer IH. Prejudice and discrimination as social stressors. In: Meyer IH, Northridge ME, editors. The Health of Sexual Minorities. Boston, MA: Springer; 2007:242–267. doi:10.1007/978-0-387-31334-4_10
92. Hatzenbuehler ML, Pachankis JE. Stigma and minority stress as social determinants of health among lesbian, gay, bisexual, and transgender youth: research evidence and clinical implications. Pediatr Clin North Am. 2016;63(6):985–997. doi:10.1016/j.pcl.2016.07.003
93. Hughto JMW, Quinn EK, Dunbar MS, Rose AJ, Shireman TI, Jasuja GK. Prevalence and co-occurrence of alcohol, nicotine, and other substance use disorder diagnoses among US transgender and cisgender adults. JAMA Netw Open. 2021;4(2):e2036512. doi:10.1001/jamanetworkopen.2020.36512
94. Peralta RL, Victory E, Thompson CL. Alcohol use disorder in sexual minority adults: age- and sex- specific prevalence estimates from a national survey, 2015–2017. Drug Alcohol Depend. 2019;205:107673. doi:10.1016/j.drugalcdep.2019.107673
95. Schuler MS, Collins RL. Sexual minority substance use disparities: bisexual women at elevated risk relative to other sexual minority groups. Drug Alcohol Depend. 2020;206:107755. doi:10.1016/j.drugalcdep.2019.107755
96. Paschen-Wolff MM, Velasquez R, Aydinoglo N, Campbell ANC. Simulating the experience of searching for LGBTQ-specific opioid use disorder treatment in the United States. J Subst Abuse Treat. 2022;140:108828. doi:10.1016/j.jsat.2022.108828
97. Braunstein MD. The five stages of LGBTQ discrimination and its effects on mass incarceration. U Miami Race Soc Just L Rev. 2017;7:217–246.
98. Girouard MP, Goldhammer H, Keuroghlian AS. Understanding and treating opioid use disorders in lesbian, gay, bisexual, transgender, and queer populations. Subst Abus. 2019;40(3):335–339. doi:10.1080/08897077.2018.1544963
99. Gardner EM, McLees MP, Steiner JF, Del Rio C, Burman WJ. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clin Infect Dis. 2011;52(6):793–800. doi:10.1093/cid/ciq243
100. Belenko S, Knight D, Wasserman GA, et al. The Juvenile Justice Behavioral Health Services Cascade: a new framework for measuring unmet substance use treatment services needs among adolescent offenders. J Subst Abuse Treat. 2017;74:80–91. doi:10.1016/j.jsat.2016.12.012
101. Knight DK, Belenko S, Dennis ML, et al. The comparative effectiveness of Core versus Core+Enhanced implementation strategies in a randomized controlled trial to improve substance use treatment receipt among justice-involved youth. BMC Health Serv Res. 2022;22(1):1535. doi:10.1186/s12913-022-08902-6
102. Williams A, Nunes E, Olfson M. To battle the opioid overdose epidemic, deploy the ‘cascade of care’ model. Health Affairs; March 13, 2017. Available from: https://www.healthaffairs.org/content/forefront/battle-opioid-overdose-epidemic-deploy-cascade-care-model.
103. Scott CK, Dennis ML, Grella CE, Mischel AF, Carnevale J. The impact of the opioid crisis on US state prison systems. Health Justice. 2021;9(17):1–16.
104. Zaller N, Donadeo K, Coffey J, Zielinski M, Brinkley-Rubinstein L. Screening for opioid use disorder in the largest jail in Arkansas: a brief report. J Correct Health Care. 2019;25(3):214–218. doi:10.1177/1078345819852133
105. Humeniuk R, Ali R. Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) and pilot brief intervention: a technical report of Phase II findings of the WHO ASSIST Project. World Health Organization; 2006. Available from: https://apps.who.int/iris/handle/10665/43504.
106. [NIDA] National Institute on Drug Abuse (2009). NIDA modified-ASSIST; July 20, 2023. Available from: https://nida.nih.gov/sites/default/files/pdf/nmassist.pdf.
107. Staton M, Tillson M, Levi MM, Webster JM, Oser CB, Leukefeld C. Screening incarcerated women for opioid use disorder (OUD). J Drug Issues. 2023. doi:10.1177/00220426231151595
108. Wolff N, Shi J. Screening for substance use disorder among incarcerated men with the Alcohol, Smoking, Substance Involvement Screening Test (ASSIST): a comparative analysis of computer-administered and interviewer-administered modalities. J Subst Abuse Treat. 2015;53:22–32. doi:10.1016/j.jsat.2015.01.006
109. Dawson‐Rose C, Shehadeh D, Hao J, et al. Trauma, substance use, and mental health symptoms in transitional age youth experiencing homelessness. Public Health Nurs. 2020;37(3):363–370. doi:10.1111/phn.12727
110. Shuper PA, Joharchi N, Bogoch II, et al. Alcohol consumption, substance use, and depression in relation to HIV Pre-Exposure Prophylaxis (PrEP) nonadherence among gay, bisexual, and other men-who-have-sex-with-men. BMC Public Health. 2020;20(1):1782–1782. doi:10.1186/s12889-020-09883-z
111. Lee CT, Lin CY, Koós M, et al. The eleven-item Alcohol, Smoking and Substance Involvement Screening Test (ASSIST-11): cross- cultural psychometric evaluation across 42 countries. J Psychiatr Res. 2023;165:16–27. doi:10.1016/j.jpsychires.2023.06.033
112. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
113. Centers for Disease Control and Prevention. Module 5: assessing and addressing opioid use disorder (OUD); 2021. Available from: https://www.cdc.gov/drugoverdose/training/oud/accessible/index.html.
114. Substance Abuse and Mental Health Services Administration. Medicaid coverage of medication-assisted treatment for alcohol and opioid use disorders and of medication for the reversal of opioid overdose; November, 2018. Available from: https://store.samhsa.gov/product/Medicaid-Coverage-of-Medication-Assisted-Treatment-for-Alcohol-and-Opioid-Use-Disorders-and-of-Medication-for-the-Reversal-of-Opioid-Overdose/SMA18-5093.
115. Dela Cruz AM, Walker R, Pipes R, et al. Creation of an algorithm for clinical decision support for treatment of opioid use disorder with buprenorphine in primary care. Addict Sci Clin Pract. 2021;16(1):12. doi:10.1186/s13722-021-00222-0
116. You DS, Mardian AS, Darnall BD, et al. A brief screening tool for opioid use disorder: EMPOWER study expert consensus protocol. Front Med. 2021;8:591201. doi:10.3389/fmed.2021.591201
117. Dunn KE, Barrett FS, Fingerhood M, Bigelow GE. Opioid overdose history, risk behaviors, and knowledge in patients taking prescribed opioids for chronic pain. Pain Med. 2017;18(8):1505–1515. doi:10.1093/pm/pnw228
118. Chandler RK, Fletcher BW, Volkow ND. Treating drug abuse and addiction in the criminal justice system: improving public health and safety. JAMA. 2009;301(2):183–190. doi:10.1001/jama.2008.976
119. Inciardi JA, Martin SS, Butzin CA. Five-year outcomes of therapeutic community treatment of drug-involved offenders after release from prison. Crime Delinq. 2004;50(1):88–107. doi:10.1177/0011128703258874
120. Harrison LD, Butzin CA, Inciardi JA, Martin SS. Integrating HIV-prevention strategies in a therapeutic community work-release program for criminal offenders. Prison J. 1998;78(3):232–243. doi:10.1177/0032885598078003003
121. Lockwood D, McCorkel J, Inciardi JA. Developing comprehensive prison-based therapeutic community treatment for women. Drugs Soc. 1998;13(1–2):193–212. doi:10.1300/J023v13n01_12
122. Sacks JY, McKendrick K, Hamilton Z. A randomized clinical trial of a therapeutic community treatment for female inmates: outcomes at 6 and 12 months after prison release. J Addict Dis. 2012;31(3):258–269. doi:10.1080/10550887.2012.694601
123. Hedrich D, Alves P, Farrell M, et al. The effectiveness of opioid maintenance treatment in prison settings: a systematic review. Addict. 2011;107(3):501–517. doi:10.1111/j.1360-0443.2011.03676.x
124. Lee JD, Friedmann PD, Boney TY, et al. Extended-release naltrexone to prevent relapse among opioid dependent, criminal justice system involved adults: rationale and design of a randomized controlled effectiveness trial. Contemp Clin Trials. 2015;41:110–117. doi:10.1016/j.cct.2015.01.005
125. Lee JD, Nunes EV, Bailey GL, et al. NIDA Clinical Trials Network CTN-0051, extended-release naltrexone vs. buprenorphine for opioid treatment (X: BOT): study design and rationale. Contemp Clin Trials. 2016;50:253–264. doi:10.1016/j.cct.2016.08.004
126. Staton M, Webster JM, Leukefeld C, et al. Kentucky Women’s Justice Community Opioid Innovation Network (JCOIN): a type 1 effectiveness-implementation hybrid trial to increase utilization of medications for opioid use disorder among justice-involved women. J Subst Abuse Treat. 2021;128:108284. doi:10.1016/j.jsat.2021.108284
127. Taylor E, Timko C, Harris AHS, Yu M, Finlay AK. Receipt of pharmacotherapy for alcohol use disorder by justice-involved women in the Veterans Health Administration. Addict Sci Clin Pract. 2019;14(1):1. doi:10.1186/s13722-018-0129-x
128. Najavits L. Seeking Safety: A Treatment Manual for PTSD and Substance Abuse. New York, NY: Guilford Press; 2001.
129. Najavits LM, Hien D. Helping vulnerable populations: a comprehensive review of the treatment outcome literature on substance use disorder and PTSD. J Clin Psychol. 2013;69(5):433–479. doi:10.1002/jclp.21980
130. Lynch SM, Heath NM, Mathews KC, Cepeda GJ. Seeking safety: an intervention for trauma-exposed incarcerated women? J Trauma Dissociation. 2012;13(1):88–101. doi:10.1080/15299732.2011.608780
131. Zlotnick C, Johnson J, Najavits LM. Randomized controlled pilot study of cognitive-behavioral therapy in a sample of incarcerated women with substance use disorder and PTSD. Behav Ther. 2009;40(4):325–336. doi:10.1016/j.beth.2008.09.004
132. Henderson A, Kroese BS. Group interventions for trauma and substance misuse available for women in criminal justice services: a systematic review of the literature. J Forensic Pract. 2020;22(4):235–249. doi:10.1108/JFP-05-2020-0024
133. Johnstone S, Dela Cruz GA, Kalb N, et al. A systematic review of gender-responsive and integrated substance use disorder treatment programs for women with co-occurring disorders. Am J Drug Alcohol Abuse. 2023;49(1):21–42. doi:10.1080/00952990.2022.2130348
134. Sherman ADF, Balthazar M, Zhang W, et al. Seeking safety intervention for comorbid post-traumatic stress and substance use disorder: a meta-analysis. Brain Behav. 2023;13(5):e2999. doi:10.1002/brb3.2999
135. Covington SS, Burke C, Keaton S, Norcott C. Evaluation of a trauma-informed and gender-responsive intervention for women in drug treatment. J Psychoactive Drugs. 2008;Suppl 5:387–398. doi:10.1080/02791072.2008.10400666
136. Messina N, Calhoun S, Braithwaite J. Trauma-informed treatment decreases posttraumatic stress disorder among women offenders. J Trauma Dissociation. 2014;15(1):6–23. doi:10.1080/15299732.2013.818609
137. Riley BJ, Smith D, Baigent MF. Mindfulness and acceptance-based group therapy: an uncontrolled pragmatic pre-post pilot study in a heterogeneous population of female prisoners. Int J Offender Ther Comp Criminol. 2019;63(15–16):2572–2585. doi:10.1177/0306624X19858487
138. McKim A. Addicted to Rehab: Race, Gender, and Drugs in the Era of Mass Incarceration. New Brunswick, NJ: Rutgers University Press; 2017.
139. Morash M. Women on Probation and Parole: A Feminist Critique of Community Programs and Services. Boston: Northeastern University Press; 2010.
140. Grella CE, Ostlie E, Watson DP, Scott CK, Carnevale J, Dennis ML. Scoping review of interventions to link individuals to substance use services at discharge from jail. J Subst Abuse Treat. 2022;138:108718. doi:10.1016/j.jsat.2021.108718
141. Zweben JE. Women’s treatment in criminal justice settings. In: Leukefeld C, Gulotta TP, Gregrich J, editors. Handbook of Evidence-Based Substance Abuse Treatment in Criminal Justice Settings. New York: Springer; 2011:229–244.
142. Bunting AM, Oser C, Staton M, Knudsen H. Polysubstance use patterns among justice-involved individuals who use opioids. Subst Use Misuse. 2020;55(13):2165–2174. doi:10.1080/10826084.2020.1795683
143. Zgoba KM, Reeves R, Tamburello A, Debilio L. Criminal recidivism in inmates with mental illness and substance use disorders. J Am Acad Psychiatry Law. 2020;48(2):209–215. doi:10.29158/JAAPL.003913-20
144. Pizzicato LN, Drake R, Domer-Shank R, Johnson CC, Viner KM. Beyond the walls: risk factors for overdose mortality following release from the Philadelphia Department of Prisons. Drug Alcohol Depend. 2018;189:108–115. doi:10.1016/j.drugalcdep.2018.04.034
145. Binswanger IA, Blatchford PJ, Mueller SR, Stern MF. Mortality after prison release: opioid overdose and other causes of death, risk factors, and time trends from 1999 to 2009. Ann Intern Med. 2013;159(9):592–600. doi:10.7326/0003-4819-159-9-201311050-00005
146. Ataiants J, Mazzella S, Roth AM, Robinson LF, Sell RL, Lankenau SE. Multiple victimizations and overdose among women with a history of illicit drug use. J Interpers Violence. 2022;37(3–4):NP1588–NP1613. doi:10.1177/0886260520927501
147. Scheidell JD, Hoff L, Khan MR, Bennett AS, Elliott L. Parenting and childcare responsibilities, harm reduction service engagement, and opioid overdose among women and men who use illicit opioids in New York City. Drug Alcohol Depend Rep. 2022;3. doi:10.1016/j.dadr.2022.100054
148. Jason LA, Salomon-Amend M, Guerrero M, Bobak T, O’Brien J, Soto-Nevarez A. The emergence, role, and impact of recovery support services. Alcohol Res. 2021;41(1):04. doi:10.35946/arcr.v41.1.04
149. Reingle Gonzalez JM, Rana RE, Jetelina KK, Roberts MH. The value of lived experience with the criminal justice system: a qualitative study of peer re-entry specialists. Int J Offender Ther Comp Criminol. 2019;63(10):1861–1875. doi:10.1177/0306624X19830596
150. Stack E, Hildebran C, Leichtling G, et al. Peer recovery support services across the continuum: in community, hospital, corrections, and treatment and recovery agency settings – a narrative review. J Addict Med. 2022;16(1):93–100. doi:10.1097/ADM.0000000000000810
151. Substance Abuse and Mental Health Services Administration. Guidelines for successful transition of people with mental or substance use disorders from jail and prison: implementation guide. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2017. Available from: https://store.samhsa.gov/product/Guidelines-for-Successful-Transition-of-People-with-Mental-or-Substance-Use-Disorders-from-Jail-and-Prison-Implementation-Guide/SMA16-4998.
152. Heidemann G, Cederbaum JA, Martinez S. “We walk through it together”: the importance of peer support for formerly incarcerated women’s success. J Offender Rehabil. 2014;53(7):522–542. doi:10.1080/10509674.2014.944741
153. Tillson M, Fallin-Bennett A, Staton M. Providing peer navigation services to women with a history of opioid misuse pre- and post-release from jail: a program description. J Clin Transl Sci. 2022;6(1):e106. doi:10.1017/cts.2022.441
154. Cobbina JE, Huebner BM, Berg MT. Men, women, and postrelease offending: an examination of the nature of the link between relational ties and recidivism. Crime Delinq. 2012;58(3):331–361. doi:10.1177/0011128710382348
155. Snell-Rood C, Staton-Tindall M, Victor G. Incarcerated women’s relationship-based strategies to avoid drug use after community re-entry. Women Health. 2016;56(7):843–858. doi:10.1080/03630242.2015.1118732
156. Johnson IM. Women parolees’ perceptions of parole experiences and parole officers. Am J Crim Justice. 2015;40(4):785–810. doi:10.1007/s12103-014-9284-0
157. Morash M, Kashy DA, Smith SW, Cobbina JE. The effects of probation or parole agent relationship style and women offenders’ criminogenic needs on offenders’ responses to supervision interactions. Crim Justice Behav. 2015;42(4):412–434. doi:10.1177/0093854814551602
158. Miller HV. Female re-entry and gender-responsive programming. U.S. Department of Justice, Office of Justice Programs, National Institute of Justice; 2021. Available from: https://nij.ojp.gov/topics/articles/female-reentry-and-gender-responsive-programming.
159. Marsden J, Stillwell G, Jones H, et al. Does exposure to opioid substitution treatment in prison reduce the risk of death after release? A national prospective observational study in England. Addict. 2017;112(8):1408–1418. doi:10.1111/add.13779
160. Evans EA, Wilson D, Friedmann PD. Recidivism and mortality after in-jail buprenorphine treatment for opioid use disorder. Drug Alcohol Depend. 2022;231:109254. doi:10.1016/j.drugalcdep.2021.109254
161. Gan WQ, Kinner SA, Nicholls TL, et al. Risk of overdose-related death for people with a history of incarceration. Addict. 2021;116(6):1460–1471. doi:10.1111/add.15293
162. Park TW, Larochelle MR, Saitz R, Wang N, Bernson D, Walley AY. Associations between prescribed benzodiazepines, overdose death and buprenorphine discontinuation among people receiving buprenorphine. Addict. 2020;115(5):924–932. doi:10.1111/add.14886
163. Ranapurwala SI, Shanahan ME, Alexandridis AA, et al. Opioid overdose mortality among former North Carolina inmates: 2000–2015. Am J Public Health. 2018;108(9):1207–1213. doi:10.2105/AJPH.2018.304514
164. El-Bassel N, Marotta PL, Goddard-Eckrich D, et al. Drug overdose among women in intimate relationships: the role of partner violence, adversity and relationship dependencies. PLoS One. 2019;14(12):e0225854. doi:10.1371/journal.pone.0225854
165. Thumath M, Humphreys D, Barlow J, et al. Overdose among mothers: the association between child removal and unintentional drug overdose in a longitudinal cohort of marginalised women in Canada. Int J Drug Policy. 2021;91:102977. doi:10.1016/j.drugpo.2020.102977
This post was originally published on this site be sure to check out more of their content.



